
Cervicogenic headaches originate in the neck, not the head. They’re caused by dysfunction in the upper cervical spine, and they respond well to targeted manual therapy and exercise, often resolving completely when the underlying neck problem is treated.
That distinction changes everything. If you’ve been treating your headaches as migraines or tension headaches without improvement, there’s a real possibility the source is your neck.
How do you know a headache is coming from your neck?
The pattern is distinctive once you know what to look for. Pain typically starts at the base of the skull or in the upper neck, then radiates forward to the forehead, temple, or around the eye. It’s almost always one-sided, though the side can occasionally alternate. Moving your neck, particularly looking upward or rotating to one side, provokes or worsens the pain.
A patient might sit at a desk all morning feeling fine, then turn to speak to a colleague and feel a dull ache spread from the back of the neck over the top of the skull. That’s textbook cervicogenic headache. Stiffness in the neck usually accompanies the pain, and pressing on specific points at the base of the skull often reproduces the familiar headache.
Cervicogenic headaches account for an estimated 2.2% of headache presentations in the general population (Antonaci et al., Current Neurology and Neuroscience Reports, 2011). They’re far more common than most people realise, and they’re frequently misdiagnosed as migraines or tension-type headaches because the pain location overlaps.
What’s actually happening in the neck?
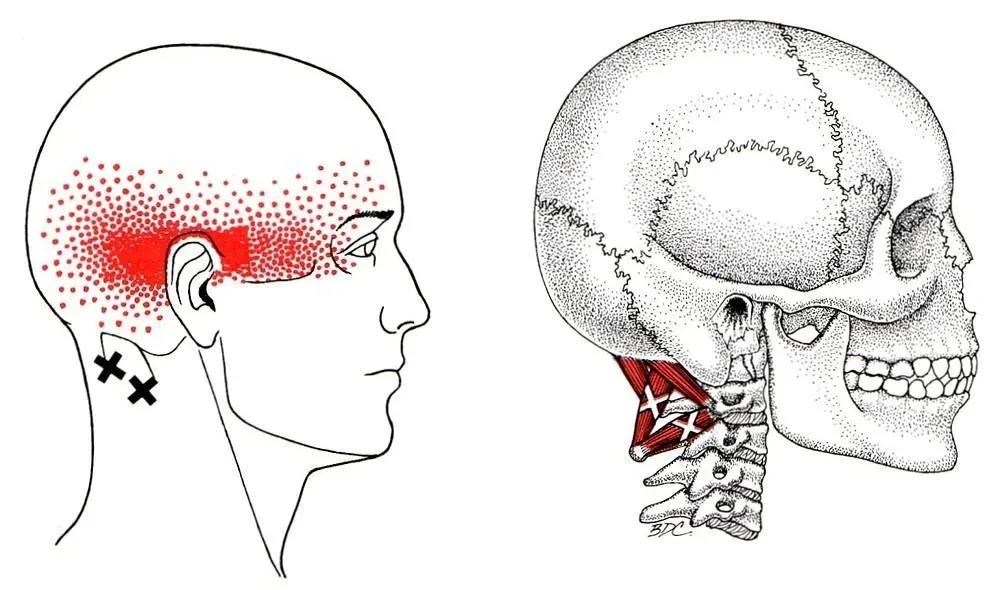
The upper three cervical vertebrae (C1, C2, and C3) share nerve pathways with the trigeminal nerve, which supplies sensation to the face and head. This convergence in the trigeminocervical nucleus means that irritation in the upper neck can be felt as pain in the head. It’s referred pain, the same principle that makes a heart attack cause arm pain.
Joint stiffness, muscle tightness, or disc problems in the upper cervical spine can all trigger this referral pattern. Whiplash injuries are a common precipitant. So is sustained poor posture, particularly the forward-head position that comes from hours at a screen. The joints stiffen, the suboccipital muscles shorten, and the nerve roots at C2 and C3 become irritated.
An edge case worth knowing: cervicogenic headaches can coexist with migraines. Someone might have both, with the neck dysfunction lowering the threshold for migraine attacks. Treating the cervicogenic component often reduces migraine frequency as well, even if it doesn’t eliminate migraines entirely.
How are cervicogenic headaches diagnosed?
There’s no single definitive test. Diagnosis relies on a combination of clinical findings: one-sided headache triggered by neck movement or pressure on the cervical spine, reduced neck range of motion, and pain that starts in the neck and spreads to the head. The International Headache Society criteria require that the headache resolves when the cervical source is treated, which is both a diagnostic criterion and a therapeutic test.
Imaging such as MRI or X-ray can rule out serious pathology but won’t confirm a cervicogenic headache on its own. Many people have cervical disc degeneration on MRI without any headaches at all. Clinical examination remains the gold standard.
At Costa Health, the assessment includes specific palpation of the upper cervical joints, range of motion testing, and provocation tests designed to reproduce the headache pattern. This hands-on approach identifies the exact spinal level and tissue responsible.
What treatments work for cervicogenic headaches?
A 2019 Cochrane review found that manual therapy combined with exercise produced greater reductions in headache frequency and intensity than exercise alone (Defined by Gross et al., Cochrane Database of Systematic Reviews). The key word is “combined.” Hands-on treatment gets things moving; exercise keeps them moving.
Physiotherapy targets the specific cervical segments involved. Flora Muijzer, trained in McKenzie MDT, uses directional preference assessment to determine which movements reduce symptoms, then prescribes a focused home exercise programme. Strengthening the deep neck flexors, the small stabilising muscles at the front of the cervical spine, has strong evidence for preventing recurrence (Jull et al., Cephalalgia, 2002).
Chiropractic cervical adjustments restore segmental mobility to restricted upper cervical joints. When C1 or C2 aren’t moving properly, surrounding muscles compensate by tightening, perpetuating the cycle. A precise adjustment breaks that cycle quickly.
Osteopathy considers the broader picture. Thoracic spine stiffness often contributes to excessive strain on the cervical spine. Improving mid-back mobility reduces the demand on the neck, and cranial techniques may help in cases with longstanding symptoms.
Sports massage addresses the muscular component directly. The suboccipital muscles, upper trapezius, and sternocleidomastoid all become hypertonic in cervicogenic headache patients. Releasing this tension provides relief and improves the effectiveness of joint-focused treatments.
Can screen time really cause these headaches?
Yes, and the mechanism is straightforward. Forward-head posture increases the load on the upper cervical spine by up to 27 kg at 60 degrees of flexion (Hansraj, Surgical Technology International, 2014). Over hours, this sustained load stiffens the joints, tightens the muscles, and irritates the nerves. It’s not the screen itself but the posture adopted while using it.
Practical changes make a difference. Positioning screens at eye level, taking regular breaks, and performing chin tuck exercises throughout the day all reduce cervical load. These aren’t optional extras for people prone to cervicogenic headaches. They’re core prevention.
When should you seek urgent care?
Most cervicogenic headaches are mechanical and benign. But sudden, severe headache unlike anything experienced before, headache with fever and stiff neck, or headache following head trauma all require immediate medical assessment to rule out serious causes such as meningitis, subarachnoid haemorrhage, or intracranial pathology.
If your headaches have been gradually worsening over weeks despite treatment, or if you notice visual disturbances, speech changes, or weakness, seek medical review promptly.
Costa Health’s multidisciplinary team in Marbella and Riviera del Sol specialises in identifying and treating the cervical source of headaches. Book an appointment to find out whether your headaches are coming from your neck and what can be done about them.