
Shin splints, clinically known as medial tibial stress syndrome (MTSS), produce a diffuse, aching pain along the inner border of the shinbone during and after weight-bearing exercise. They’re the most common cause of exercise-related lower leg pain, with systematic reviews reporting incidence ranging from 7% to 35% in military and athletic populations.
That prevalence figure is striking. One in five runners will experience this at some point. Yet shin splints remain poorly understood by many of the people who get them, often dismissed as something to “run through” or treated with nothing more than ice and hope. Neither approach works reliably.
What causes the pain?
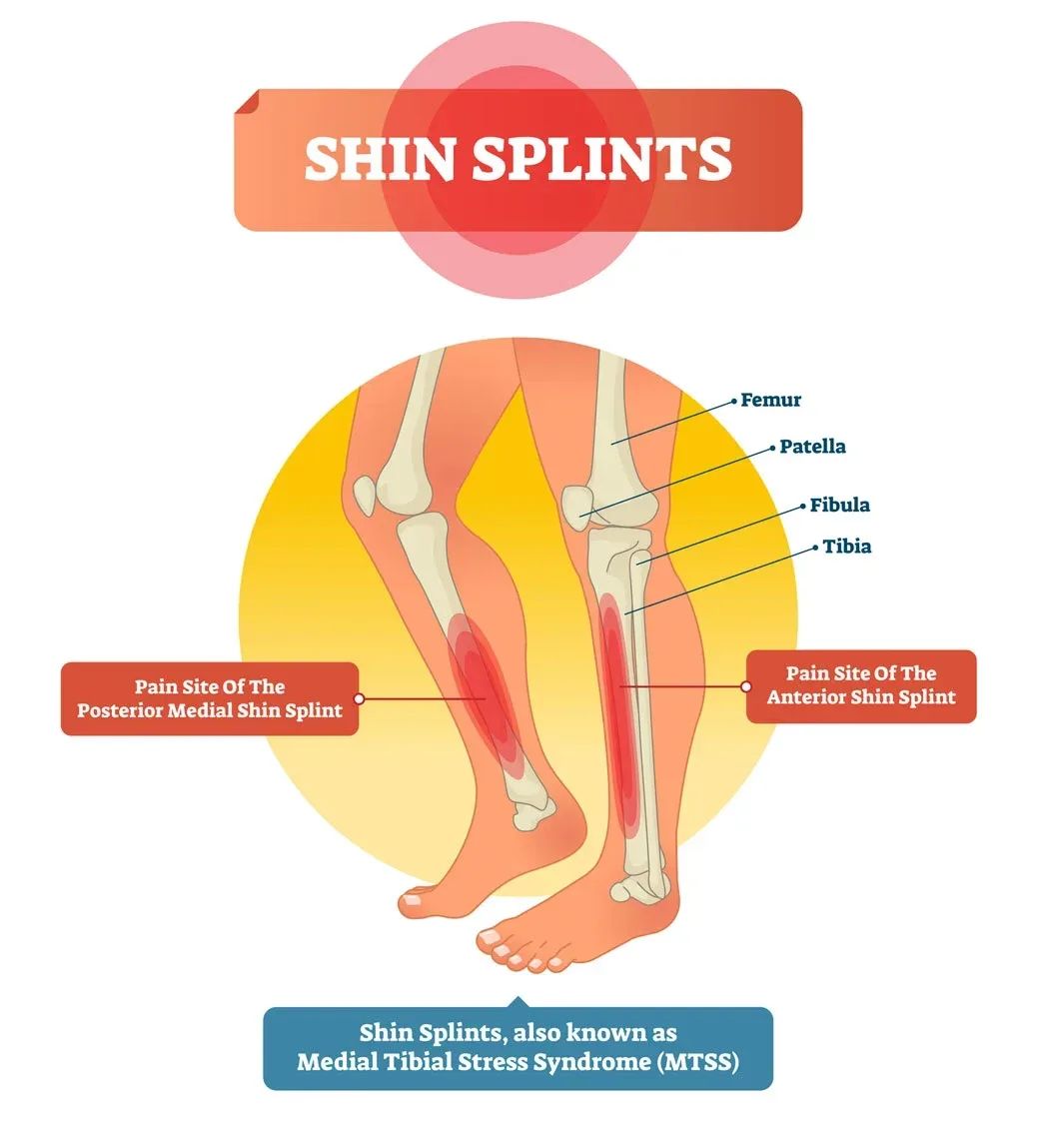
The medial tibial stress syndrome label describes what happens rather well. Repetitive loading through the tibia creates stress at the bone-periosteum junction along the posteromedial border of the shin. The periosteum, a thin membrane covering the bone, becomes irritated where muscles such as the soleus and tibialis posterior exert traction on it during foot strike.
Think of it as a tug-of-war between muscle pull and bone resistance. When training volume exceeds the bone’s adaptive capacity, microdamage accumulates faster than remodelling can repair it. The result is pain that’s initially present only during exercise, then lingers afterwards, and eventually shows up during everyday walking if left untreated.
A common misconception is that shin splints are a muscle problem. They aren’t, primarily. The muscular component exists, tight and overworked calf muscles certainly contribute, but the core pathology sits at the bone and its covering. This matters because treatment aimed purely at muscles misses the point.
Who’s at risk?
Runners top the list, particularly those who’ve recently increased their mileage, switched to harder surfaces, or started running in worn-out shoes. Dancers, military personnel, and court sport athletes (tennis, padel, basketball) follow close behind. On the Costa del Sol, Sarah Monaghan at Costa Health regularly treats expats who’ve taken up running on Marbella’s paseo maritimo, a beautiful but unforgiving concrete surface.
Biomechanical risk factors include overpronation, flat feet, leg length discrepancy, and weak hip abductors that allow excessive tibial internal rotation. Female sex is an independent risk factor, with women approximately 1.5 to 3.5 times more likely to develop MTSS than men (Yates & White, British Journal of Sports Medicine, 2004).
Body mass index matters too. Higher loads through the lower limb with every step mean more stress on the periosteum. Bone density plays a role: runners with lower bone mineral density in the tibia are more susceptible, which is one reason shin splints are more common in female athletes who may have relative energy deficiency in sport (RED-S).
How do you tell shin splints from a stress fracture?
This is the critical clinical question, and getting it wrong has real consequences. Shin splints produce diffuse tenderness along a broad area (typically five centimetres or more) of the inner shin. Stress fractures produce focal point tenderness, often over a one to two centimetre area, and the pain worsens progressively even with reduced activity.
Percussion testing, tapping the bone above or below the tender spot, may refer pain to the fracture site. The “hop test,” asking the patient to hop on the affected leg, typically provokes sharp localised pain with a stress fracture but diffuse discomfort with shin splints.
When clinical examination raises doubt, MRI is the gold standard for differentiating the two. Continuing to train on an undiagnosed tibial stress fracture risks complete fracture, which is why any shin pain that worsens despite reduced training load warrants proper investigation.
What treatment works?
Shin splints respond well to a structured, multidisciplinary approach. Costa Health’s practitioners use chiropractic, physiotherapy, osteopathy, and sports massage in combination, because addressing both the local tissue irritation and the underlying biomechanical drivers produces faster and more lasting results.
Physiotherapy forms the rehabilitation backbone. Graduated loading programmes respect the bone’s need for progressive adaptation. Tibialis posterior strengthening, calf raises (both straight and bent knee to target soleus), and hip abductor work address the muscular deficiencies that increase tibial stress. Gait retraining, particularly increasing cadence by 5-10%, reduces impact forces per stride and has strong evidence behind it.
Chiropractic assessment identifies restrictions in the ankle, subtalar, and midfoot joints that force compensatory movement patterns. Restoring full dorsiflexion at the ankle reduces the demand on the posterior compartment muscles during gait. Pelvic and lumbar assessment ensures that asymmetries further up the chain aren’t driving uneven lower limb loading.
Osteopathic treatment takes a broader view of the kinetic chain. Fascial restrictions through the lower limb, hip mobility deficits, and thoracolumbar compensations all influence how force transmits through the tibia. Addressing these wider patterns often explains why shin splints keep returning despite local treatment alone.
Sports massage targets the gastrocnemius, soleus, tibialis posterior, and peroneals, releasing chronic tension that maintains excessive periosteal traction. Myofascial release techniques applied to the posterior and deep posterior compartments provide measurable relief and improved tissue extensibility.
What can you do at home?
Relative rest, not absolute rest, is the principle. Switching from running to cycling, swimming, or elliptical training maintains fitness while reducing tibial impact loading. Ice massage along the shin for 10 minutes after activity helps manage acute symptoms. Calf stretching (wall stretches held for 30 seconds, three repetitions, three times daily) and toe raises on a step form the minimum effective home programme.
Footwear matters enormously. Shoes should be replaced every 500-800 kilometres. Motion control shoes may help overpronators, though evidence for specific shoe types is weaker than the running industry would like you to believe. Custom orthotics prescribed after proper biomechanical assessment offer a more targeted solution.
When should you worry?
Night pain that wakes you from sleep is a red flag and may indicate a stress fracture or, rarely, a bone pathology requiring urgent investigation. Localised swelling and warmth over a small area of the shin should prompt imaging. Pain that doesn’t ease at all with a week of relative rest needs professional assessment rather than continued self-management.
Recovery from straightforward shin splints typically takes four to eight weeks with appropriate treatment and load modification. Returning to full activity should follow a graded programme, increasing running volume by no more than 10% per week. Costa Health’s team can guide that return, adjusting the treatment approach as the shin heals and tolerates increasing load.