
Rotator cuff tendinitis is irritation or inflammation of one or more of the four tendons that form the rotator cuff, most commonly the supraspinatus. It produces pain in the shoulder, particularly during overhead reaching, lifting, or lying on the affected side at night. With appropriate loading strategies and rehabilitation, the vast majority of rotator cuff tendinitis cases resolve without surgery.
What is the rotator cuff and why does it matter?
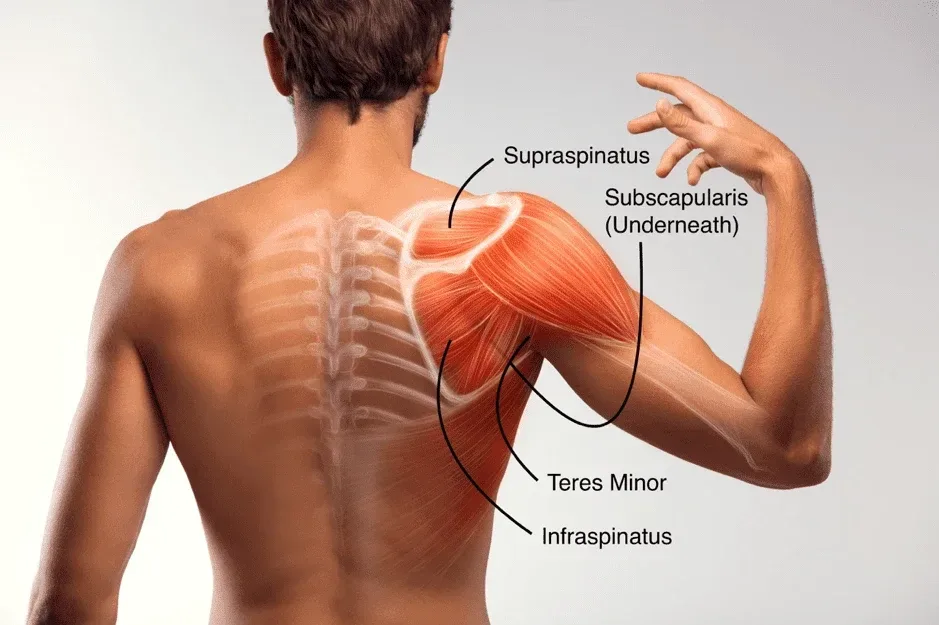
The rotator cuff is a group of four muscles, supraspinatus, infraspinatus, teres minor, and subscapularis, whose tendons wrap around the head of the humerus like a cuff. Their job isn’t just to rotate the arm. They compress and stabilise the humeral head in the shallow glenoid socket during every shoulder movement, acting as dynamic centralisers.
When these tendons become irritated, the shoulder loses its smooth, coordinated movement. People start hiking the shoulder, shrugging, or avoiding certain ranges entirely. These compensatory patterns often make the problem worse over time because they change the mechanical environment the tendons work in.
What causes rotator cuff tendinitis?
The old explanation was purely mechanical: the tendon gets pinched between the humeral head and the acromion (the bony projection above the shoulder). This “impingement” model dominated for decades. Current evidence paints a more complex picture.
Tendon irritation usually results from a mismatch between load and capacity. A weekend painter doing eight hours of overhead work, a swimmer increasing training volume before a competition, or someone returning to the gym after months of inactivity, these are the clinical scenarios Costa Health sees regularly at the Marbella and Riviera del Sol clinics. The tendon is asked to do more than it’s conditioned to handle, and it responds with pain and inflammation.
Age is a factor, but not in the way many people assume. A study by Yamamoto et al. (2010) using ultrasound screening found that rotator cuff tears are present in 20.7% of the general population, with prevalence increasing with age, yet many of these tears were completely pain-free (Yamamoto et al., 2010, J Shoulder Elbow Surg). This finding is significant because it means structural changes on imaging don’t automatically explain someone’s pain. The clinical picture, not just the scan, should guide treatment.
How can you tell if it’s the rotator cuff?
Pain on the outer aspect of the shoulder, sometimes radiating to the mid-upper arm, is the hallmark symptom. It’s often worst during specific movements: reaching overhead, putting on a coat, fastening a seatbelt, or reaching behind the back. Night pain is common, particularly when lying on the affected side, because the shoulder compresses the irritated tendon against the mattress.
A common misconception is that all shoulder pain is rotator cuff related. Neck problems, particularly from the C5 and C6 nerve roots, can refer pain into exactly the same area. Acromioclavicular joint irritation sits right next door and mimics rotator cuff symptoms during overhead pressing. Proper clinical assessment distinguishes between these, and Daniele Delicati at Costa Health routinely screens the cervical spine during any shoulder examination for this reason.
What does effective treatment involve?
Exercise-based rehabilitation is the first-line treatment and the approach best supported by research. A well-designed programme progressively loads the rotator cuff tendons, rebuilds the strength and endurance that was lost, and restores confident, pain-free shoulder movement.
Physiotherapy for rotator cuff tendinitis typically begins with isometric exercises, where the muscle contracts without the joint moving. Isometrics are useful early on because they can reduce pain while beginning the strengthening process. From there, the programme progresses to isotonic exercises through range, scapular stability work, and eventually functional or sport-specific loading.
Chiropractic and osteopathic assessment of the thoracic spine and ribcage is an often overlooked piece. Thoracic stiffness limits scapular movement, and the scapula is the foundation the rotator cuff works from. If the foundation isn’t moving well, the rotator cuff is always working at a disadvantage. Manual therapy directed at thoracic mobility can produce immediate improvements in overhead range.
Sports massage addresses the muscular tightness that develops in the upper trapezius, levator scapulae, and pectorals as the body compensates for shoulder pain. Releasing these areas doesn’t fix the tendon itself, but it creates a better environment for rehabilitation exercises to be performed correctly.
Should you rest a sore rotator cuff?
Complete rest is tempting but counterproductive. Tendons need load to heal and adapt. Removing all load leads to further deconditioning and often makes the pain worse when activity resumes. The evidence clearly supports relative rest, avoiding aggravating activities in the short term, while introducing a graded loading programme as soon as tolerable.
Cortisone injections can provide short-term pain relief, but repeated injections have been associated with tendon weakening. They’re best used selectively, when pain is preventing participation in rehabilitation, rather than as a standalone treatment.
When should someone seek urgent assessment?
Sudden onset of severe weakness after a fall or injury, particularly in anyone over 40, raises the possibility of an acute rotator cuff tear that may need surgical consideration. Inability to lift the arm at all, significant bruising around the shoulder, or symptoms accompanied by numbness or tingling down the arm warrant prompt assessment.
Costa Health provides thorough shoulder assessments and structured rehabilitation programmes for rotator cuff tendinitis at both the Marbella and Riviera del Sol clinics. Book a consultation to start your recovery.