
Shoulder impingement syndrome is pain that occurs when soft tissues in the shoulder, typically the rotator cuff tendons or subacromial bursa, become compressed during arm elevation. It produces a characteristic “painful arc” between roughly 60 and 120 degrees of shoulder abduction. Despite being one of the most common shoulder diagnoses, the understanding of what actually causes impingement has changed significantly in recent years, and that shift matters for treatment.
Is impingement really about “pinching”?
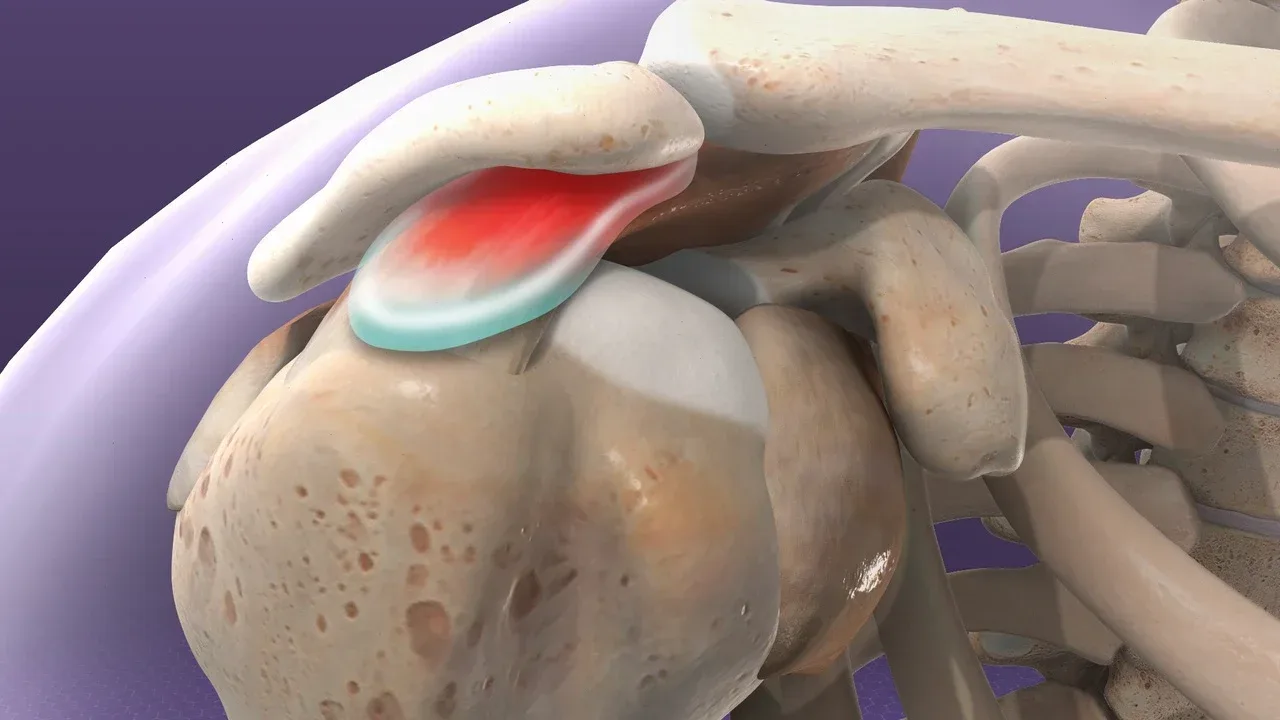
For decades, the dominant theory held that the supraspinatus tendon gets physically pinched between the humeral head and the acromion during overhead movement. Charles Neer proposed this model in 1972, and it led to thousands of acromioplasty surgeries, procedures that shave bone from the acromion to create more space.
The problem is that the evidence has moved on. A landmark randomised controlled trial published in The Lancet (the CSAW trial) found that arthroscopic subacromial decompression was no more effective than a placebo (sham) surgery for shoulder impingement (Beard et al., 2018, The Lancet). Both groups improved, but so did the group that received no surgery at all. This strongly suggests that the mechanical “pinching” model is incomplete at best.
Current thinking frames impingement as a clinical presentation rather than a single pathological process. The pain likely arises from a combination of tendon irritation, bursal inflammation, altered motor control, and load management errors. Understanding this distinction is important because it shifts the treatment focus from “creating more space” to addressing why the tissues became sensitised in the first place.
What does shoulder impingement feel like?
Pain on the outer shoulder during arm elevation is the hallmark. Reaching overhead to a high shelf, putting on a shirt, or swimming front crawl tend to provoke it. The painful arc, where the middle range of shoulder elevation is painful but full elevation above the head may actually feel better, is a distinctive feature.
Night pain is common. Lying on the affected side compresses the shoulder structures, and many people find they wake repeatedly or can only sleep on the opposite side. Stiffness in the morning that loosens with gentle movement is typical, distinguishing impingement from a frozen shoulder where stiffness is persistent and progressive.
A clinical example from practice: a 52-year-old recreational swimmer attending Costa Health’s Marbella clinic presented with six weeks of progressively worsening shoulder pain during front crawl. Assessment revealed not just subacromial tenderness but significant thoracic spine stiffness and weakness in the lower trapezius and serratus anterior, muscles responsible for controlling the shoulder blade during overhead movement. Treating the shoulder in isolation would have missed half the problem.
Why does impingement develop?
Training load errors are the most common trigger. Painters, decorators, swimmers, tennis players, and gym-goers who suddenly increase overhead volume are the classic profiles. The supraspinatus tendon and subacromial bursa are asked to handle more repetitive compression than they’re conditioned for, and they respond with inflammation and pain.
Scapular dyskinesis, abnormal shoulder blade movement, is frequently found alongside impingement symptoms. When the scapula doesn’t upwardly rotate and posteriorly tilt sufficiently during arm elevation, the subacromial space narrows dynamically. This isn’t a structural problem. It’s a motor control and strength problem, and it’s treatable.
Thoracic spine stiffness is another major contributor that’s often overlooked. The thoracic spine needs to extend as the arm goes overhead. A stiff, kyphotic thoracic spine limits this, forcing the shoulder to compensate. This is particularly relevant for office workers and anyone who spends hours in a forward-leaning posture.
How is impingement syndrome treated?
Exercise-based rehabilitation targeting the rotator cuff and scapular stabilisers is the first-line treatment, and the evidence strongly supports it over passive interventions. Multiple systematic reviews, including a 2019 Cochrane review (Karjalainen et al.) and a 2020 update in JOSPT (Shire et al.), found strong evidence that exercise therapy is as effective as surgery for subacromial impingement, with lower risk and cost.
Physiotherapy at Costa Health focuses on a progressive loading programme. Early phases address pain management through isometric rotator cuff exercises and manual therapy. Daniele Delicati integrates thoracic mobilisation and scapular control work from the outset, because the shoulder blade and the mid-back are inseparable from shoulder function.
Osteopathic and chiropractic approaches to the thoracic spine and rib articulations can restore the extension and rotation needed for pain-free overhead movement. These manual techniques work best when combined with an active exercise programme rather than used in isolation.
Sports massage addresses secondary muscle tightness in the pectorals, upper trapezius, and latissimus dorsi that develops as the body compensates for shoulder pain. Reducing this guarding helps patients perform their rehabilitation exercises through the correct movement patterns.
Does impingement go away on its own?
Mild cases sometimes settle with activity modification alone. However, without addressing the underlying scapular control, rotator cuff capacity, and thoracic mobility deficits, recurrence is common, particularly when people return to the activity that triggered it.
When should someone seek assessment?
Shoulder pain lasting more than two weeks, night pain that disrupts sleep, or pain during daily activities like dressing and reaching overhead all warrant professional assessment. Sudden severe weakness or an inability to lift the arm after a fall or trauma raises the possibility of a rotator cuff tear and needs prompt evaluation.
Costa Health’s team in Marbella and Riviera del Sol provides thorough shoulder assessments and structured, evidence-based rehabilitation for impingement and rotator cuff tendinitis. Book a consultation to get a clear diagnosis and start treatment.