
Cervical facet syndrome is pain originating from the small zygapophyseal joints on either side of the cervical spine. It produces a deep, aching neck pain that’s often felt on one side and can refer pain into the shoulder blade, the back of the skull, or behind the ear. It’s one of the most underdiagnosed sources of neck pain, frequently mistaken for muscular strain or cervical disc herniation.
What causes the cervical facet joints to become painful?
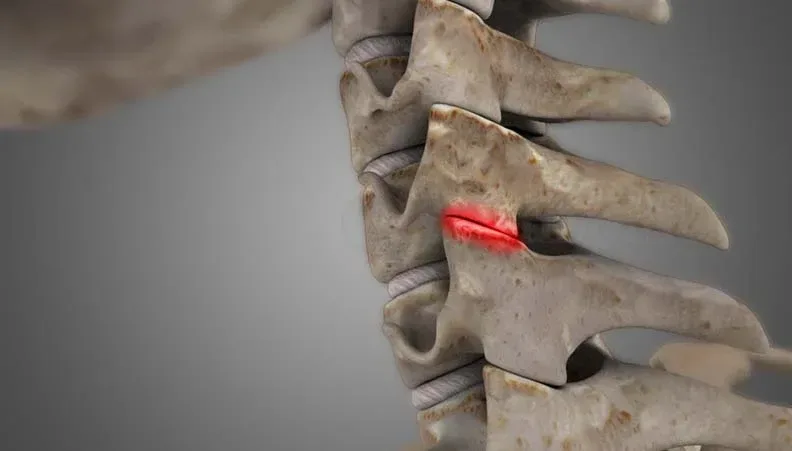
The cervical facets guide rotation and side-bending of the neck. They’re load-bearing joints lined with cartilage, wrapped in a capsule rich in nerve endings, and surrounded by a meniscoid fold that can become trapped during sudden movements. Any of these structures can generate pain.
Whiplash is one of the most thoroughly documented causes. Research using controlled diagnostic nerve blocks consistently identifies the cervical facet joints as the pain source in 36% to 67% of chronic neck pain patients. A 2020 study in Pain Physician (Manchikanti et al.) found a prevalence of 49% using a chronic pain model with controlled comparative blocks. That’s roughly half of all chronic neck pain presentations, a finding that has shaped clinical thinking for over two decades.
Age-related degeneration is the other major driver. As cervical discs lose height over time, more load transfers to the facet joints behind them. Prolonged desk work and forward-head posture accelerate this process by placing the cervical facets in sustained compression. Sarah Monaghan, chiropractor and clinic owner at Costa Health, sees this pattern constantly among expats who’ve spent decades in office-based careers before relocating to the Costa del Sol.
How do you know it’s a facet problem?
The hallmark is pain on extension and rotation to the affected side. Tipping your head back and turning it simultaneously loads the facet joints directly. If that reproduces your familiar neck pain, the facets are a likely culprit.
Referral patterns help narrow it further. The upper cervical facets (C2-C3 and C3-C4) tend to refer pain into the occiput and temple, mimicking cervicogenic headaches. The mid-cervical joints (C4-C5 and C5-C6) refer into the shoulder and scapula. These referral maps were established by Dwyer, Aprill, and Bogduk in their 1990 provocation study and remain the clinical reference point.
A common misconception is that cervical facet pain always appears after trauma. It doesn’t. Insidious onset is just as frequent. People wake up one morning unable to turn their head, with no injury, no incident, just an accumulation of poor positioning that finally tips the joint into an inflammatory state.
One edge case to watch for: the acute locked neck. Occasionally a cervical facet meniscoid fold becomes entrapped during a quick rotation, producing sudden severe pain and almost total loss of movement to one side. It looks alarming but usually responds well to skilled manual therapy within one or two sessions.
What does treatment involve?
Costa Health approaches cervical facet syndrome from multiple angles, matching the technique to the patient rather than forcing a one-size-fits-all protocol.
Chiropractic cervical manipulation remains one of the fastest ways to restore movement and reduce pain in an irritable facet joint. A precisely delivered adjustment gaps the joint surfaces, releases trapped meniscoid tissue, and triggers a neurophysiological pain-inhibitory response. It’s not appropriate for every patient, which is exactly why a thorough examination comes first.
Osteopathic approaches favour gentle articulation and muscle energy techniques. These are especially useful for patients who are anxious about neck manipulation, or for acute presentations where the tissues are too irritated for thrust techniques.
Physiotherapy builds the longer-term solution. Deep cervical flexor training, the muscles at the front of the neck that stabilise the cervical spine, has strong evidence behind it. A randomised controlled trial published in Spine (2002) showed that specific cranio-cervical flexion training significantly reduced neck pain and headache frequency over 12 months compared to general exercise alone.
Sports massage releases the upper trapezius, levator scapulae, and suboccipital muscles that invariably tighten up around an inflamed cervical facet. Reducing that muscular bracing often produces an immediate improvement in range.
When should cervical facet pain raise a red flag?
Most cervical facet syndrome responds well to conservative care within a few weeks. Serious underlying pathology is rare but needs ruling out.
Bilateral arm weakness, difficulty with fine motor tasks like buttoning a shirt, or changes in gait and balance could indicate cervical myelopathy, compression of the spinal cord itself. This is a surgical condition and requires urgent referral. Dizziness, double vision, or difficulty swallowing after a neck injury should prompt immediate medical assessment to exclude vertebral artery involvement.
If you’re experiencing persistent one-sided neck pain or headaches that conventional painkillers aren’t touching, book an appointment at Costa Health. Sarah Monaghan and the clinical team can determine whether cervical facet syndrome is the cause and get you on a targeted treatment plan.