
A cervical disc herniation occurs when the soft centre of a disc in the neck pushes through its outer wall, pressing on a nearby nerve root. Most cervical disc herniations improve significantly within 8 to 12 weeks with targeted manual therapy and exercise, without the need for surgery.
That timeline surprises most people. The pain can be severe, radiating from the neck down into the arm and hand, and it’s natural to assume something that painful must require an operation. In the vast majority of cases, it doesn’t.
What does a cervical disc herniation feel like?
The hallmark symptom is radiculopathy: sharp, burning, or electric pain that shoots from the neck into the shoulder, arm, and often the hand. The exact path depends on which disc is affected. A C5-C6 herniation typically sends pain into the thumb and index finger. A C6-C7 herniation targets the middle finger and ring finger.
Numbness and tingling in the affected arm are common. Some people notice weakness, struggling to grip objects or lift the arm overhead. Neck stiffness accompanies the arm symptoms, and looking upward or tilting the head toward the affected side usually intensifies the pain.
Here’s a clinical example that illustrates a typical presentation: a 42-year-old padel player wakes up with a stiff neck after an intense match. Over the following 48 hours, a burning pain develops down the right arm into the index finger. Gripping the racquet becomes difficult. MRI confirms a right posterolateral disc herniation at C5-C6. Within six weeks of directional preference exercises and manual therapy, the arm symptoms resolve completely, and the player returns to the court.
What causes a disc in the neck to herniate?
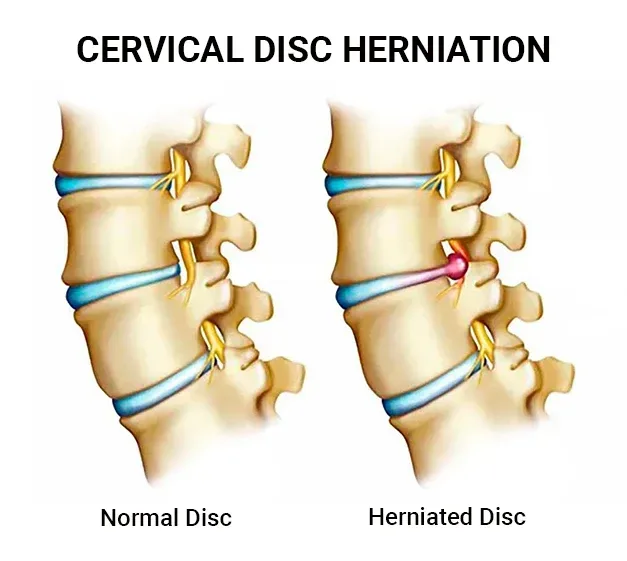
Cervical discs sit between the vertebrae, acting as shock absorbers. Each disc has a tough outer ring (the annulus fibrosus) and a softer gel-like centre (the nucleus pulposus). A herniation occurs when the annulus develops a tear and the nucleus pushes through.
Age is the primary factor. Disc degeneration begins in the late twenties, and by the age of 50, MRI studies show disc changes in over 80% of asymptomatic individuals (Brinjikji et al., AJNR, 2015). That statistic is worth sitting with. The majority of disc changes on imaging cause no symptoms at all. An MRI finding of disc herniation doesn’t automatically explain your pain, which is precisely why clinical assessment matters more than imaging.
Trauma can cause acute herniations, particularly whiplash-type injuries. Sustained poor posture, repetitive overhead work, and heavy lifting with poor mechanics also contribute. Smoking accelerates disc degeneration by impairing nutrient delivery to the disc tissue.
Do you need an MRI?
Not always, and not immediately. NICE guidelines recommend clinical assessment as the first step. If symptoms follow a clear nerve root pattern and respond to treatment within the expected timeframe, imaging is often unnecessary. MRI becomes important when symptoms persist beyond 6 to 12 weeks, when there’s progressive neurological deficit (worsening weakness), or when red flags suggest a more serious cause.
A common misconception is that a larger herniation on MRI means worse outcomes. Research shows that large disc herniations actually have a higher rate of spontaneous resorption than small ones (Chiu et al., Spine, 2015). The body’s immune system recognises the extruded disc material as foreign and gradually breaks it down. Larger herniations trigger a stronger immune response, which is why they often shrink more than smaller protrusions.
What treatments work for cervical disc herniation?
Conservative management is the first-line approach, and it’s effective for roughly 80% of patients (Carette & Fehlings, NEJM, 2005). The goal is to reduce nerve root compression, calm inflammation, and restore normal cervical mechanics.
Physiotherapy using the McKenzie MDT approach is particularly well-suited to disc herniations. Flora Muijzer at Costa Health uses directional preference assessment to find the specific movements that centralise symptoms, meaning the arm pain retreats toward the neck and eventually resolves. Repeated end-range exercises performed throughout the day progressively reduce the disc bulge’s contact with the nerve root. Strengthening the deep cervical flexors and scapular stabilisers supports long-term recovery.
Chiropractic care can address segmental hypomobility above and below the herniated level. Joints adjacent to the problem disc often become stiff as the body splints the area. Restoring mobility to these segments reduces compensatory strain and improves overall cervical function. Specific mobilisation techniques are selected based on the presentation, avoiding high-velocity manipulation at the herniated level itself.
Osteopathy considers the wider kinetic chain. Thoracic spine stiffness frequently accompanies cervical disc problems, and improving mid-back extension reduces the load on the cervical spine. Soft tissue work to the scalenes, upper trapezius, and levator scapulae muscles relieves the protective guarding that develops around the injury.
Sports massage targets the secondary muscular tension that builds up when someone has been guarding against pain for weeks. The upper back, shoulders, and forearm muscles on the affected side often develop trigger points that amplify the symptoms. Releasing this tension complements the joint-focused treatments.
When is surgery considered?
Surgery is reserved for cases that don’t respond to 6 to 12 weeks of appropriate conservative treatment, or where there’s evidence of significant or progressive neurological deficit. Anterior cervical discectomy and fusion (ACDF) is the most common procedure. It’s effective, but it isn’t risk-free and doesn’t guarantee a better outcome than continued conservative care in borderline cases.
Cervical myelopathy, where the herniation compresses the spinal cord itself rather than just a nerve root, is a different situation entirely. Symptoms include difficulty with fine motor tasks (buttoning a shirt, handwriting), unsteadiness when walking, and a feeling of clumsiness in the hands. Myelopathy requires prompt surgical referral and should not be managed with manual therapy alone.
What does recovery look like?
Most people see meaningful improvement within the first four to six weeks. Arm pain typically resolves before neck pain. The nerve takes time to recover even after the mechanical compression is reduced, so some residual numbness or tingling may persist for several months. This is normal and usually resolves fully.
Returning to activity should be graded. Overhead sports, heavy lifting, and contact activities are reintroduced progressively as strength and range of motion return. Rushing back before the supporting muscles have regained their conditioning is the most common cause of setbacks.
Long-term, maintaining good cervical posture, keeping the thoracic spine mobile, and continuing a targeted exercise programme all reduce the risk of recurrence. One herniation doesn’t condemn you to chronic problems, but it does mean the cervical spine needs ongoing attention.
Costa Health’s team in Marbella and Riviera del Sol treats cervical disc herniations across physiotherapy, chiropractic, and osteopathy, building a recovery plan around the individual presentation. Book an appointment for a thorough assessment and a clear path forward.