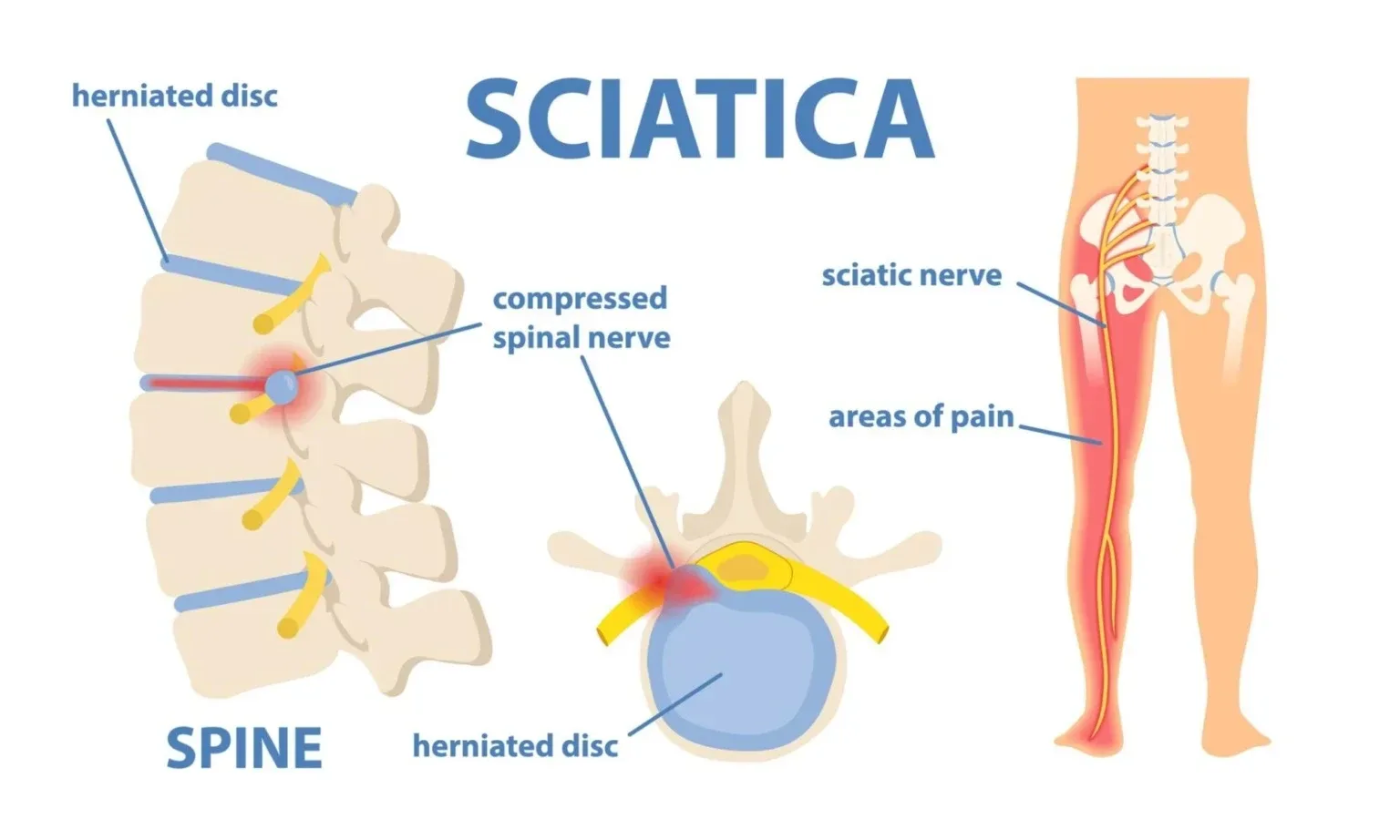

Sciatica is pain that travels along the sciatic nerve, from the lower back through the buttock and down the leg. Most cases resolve within 6 to 12 weeks with the right combination of manual therapy and guided exercise, without surgery.
That single sentence matters more than anything else on this page. If you’re reading this at 3am with burning pain down your leg, you need to know: the odds are firmly in your favour.
What does sciatica actually feel like?
The word gets thrown around loosely. Someone bends awkwardly and says “I’ve done my sciatica” when they’ve actually strained a muscle. True sciatica involves the sciatic nerve itself, the thickest nerve in the body, roughly the diameter of your little finger. When it’s compressed or irritated, you don’t just feel pain in the back. You feel it travelling.
Sharp, burning pain running from the lower back into the buttock and down the back or side of the leg is the hallmark. Some people describe it as an electric shock. Others notice numbness, pins and needles, or weakness in the foot. Sitting for long periods typically makes it worse, and coughing or sneezing can send a jolt down the leg.
A common misconception is that sciatica always means a disc problem. It doesn’t. Piriformis syndrome, where the piriformis muscle in the buttock spasms and traps the nerve, accounts for roughly 6% of sciatica cases (Hopayian et al., BMJ, 2010). Spinal stenosis, degenerative changes, and even pregnancy can all produce sciatic symptoms through different mechanisms.
What causes the sciatic nerve to become irritated?
Disc herniation in the lumbar spine is the most frequent culprit, responsible for approximately 90% of cases (NICE guideline NG59, last updated 2020). The soft inner material of a spinal disc bulges outward and presses on one of the nerve roots that form the sciatic nerve, most commonly at L4-L5 or L5-S1.
Beyond disc herniations, other causes include spinal stenosis (narrowing of the canal the nerve passes through), spondylolisthesis (where one vertebra slips forward over another), and soft tissue entrapment. Age-related wear plays a role, but sciatica isn’t just a condition of older adults. Active people in their 30s and 40s get it too, sometimes triggered by heavy lifting, prolonged sitting, or a sudden awkward movement.
Smoking increases the risk. That’s not widely known, but nicotine accelerates disc degeneration by reducing blood flow to the spinal discs (Battie et al., Spine, 2004). It’s one of the few modifiable risk factors worth mentioning.
How is sciatica diagnosed?
A thorough clinical examination usually provides the answer. The straight-leg raise test, where the clinician lifts your leg while you lie flat, is remarkably sensitive for disc-related sciatica. If it reproduces your leg pain between 30 and 70 degrees, that’s a strong indicator.
Imaging isn’t always necessary. NICE guidelines recommend against routine MRI for sciatica unless symptoms persist beyond 6 to 12 weeks, or there are red flags such as progressive weakness, loss of bladder or bowel control, or bilateral leg symptoms. These red flags, particularly cauda equina syndrome, require immediate medical attention, typically within hours.
At Costa Health, the clinical team uses a detailed history and physical examination to identify the specific mechanism driving your symptoms. Knowing whether the problem is disc-related, joint-related, or muscle-related changes the treatment approach entirely.
What treatment options work for sciatica?
The evidence strongly supports active management over bed rest. A Cochrane review (Fernandez et al., 2023) confirmed that exercise therapy combined with manual treatment produces better outcomes than passive approaches alone.
Physiotherapy forms the backbone of most sciatica treatment plans. Flora Muijzer, a McKenzie MDT-trained physiotherapist at Costa Health, uses directional preference exercises to centralise pain, meaning the leg symptoms gradually retreat toward the spine and then resolve. This approach works because it addresses the mechanical cause rather than just managing pain.
Chiropractic spinal adjustments can be highly effective when joint restriction or poor segmental mobility contributes to nerve irritation. Restoring proper movement at the affected spinal level reduces pressure on the nerve root and allows inflammation to settle.
Osteopathy takes a broader view, assessing how the pelvis, hip, and thoracic spine interact. Compensatory patterns often develop when someone has been guarding against pain for weeks, and addressing these prevents the problem from recurring.
Sports massage plays a supporting role, particularly when piriformis involvement or general muscular tension amplifies the nerve compression. Deep tissue work to the gluteal muscles and hamstrings can provide meaningful short-term relief while other treatments address the root cause.
When should you worry about sciatica?
Most sciatica is uncomfortable but not dangerous. However, certain symptoms demand urgent assessment. Loss of bladder or bowel control, numbness in the saddle area (inner thighs and perineum), or rapidly worsening weakness in both legs may indicate cauda equina syndrome, a surgical emergency. If you experience any of these, go to A&E immediately.
Progressive foot drop, where you can’t lift the front of your foot, also warrants prompt investigation. While not as urgent as cauda equina, it suggests significant nerve compression that may need intervention beyond conservative care.
Can you prevent sciatica from coming back?
Recurrence rates sit around 30% within the first year (Haugen et al., European Spine Journal, 2012). That’s a significant number, but it’s not a coin flip. Targeted rehabilitation reduces these odds. Strengthening the deep core stabilisers, improving hip mobility, and maintaining good spinal movement patterns all contribute to long-term resilience.
Prolonged sitting is a genuine risk factor. If your job keeps you at a desk, standing regularly and varying your position throughout the day makes a measurable difference. Exercise matters more than any single intervention. Walking, swimming, and Pilates all support spinal health without excessive load.
Costa Health’s team in Marbella and Riviera del Sol works across disciplines to build a recovery plan that doesn’t just resolve the current episode but reduces the chance of it returning. Book an appointment to get a clear diagnosis and a treatment plan tailored to your specific presentation.