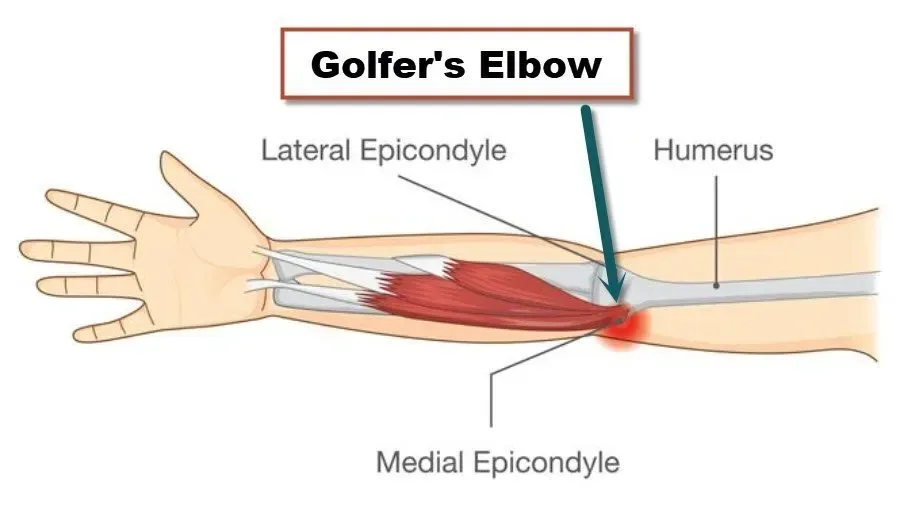

Golfer’s elbow, clinically called medial epicondylar tendinopathy, is pain on the inner side of the elbow where the forearm flexor and pronator muscles attach to the medial epicondyle. It’s a tendon overload condition that makes gripping, wrist curling, and forearm rotation painful. Like its counterpart tennis elbow, it affects far more people than its name suggests, and it responds well to progressive loading when managed correctly.
How does golfer’s elbow differ from tennis elbow?
Both are tendinopathies of the elbow, but they affect opposite sides. Tennis elbow involves the wrist extensors on the outer elbow. Golfer’s elbow involves the wrist flexors and forearm pronators on the inner elbow, specifically the common flexor tendon origin. The pronator teres and flexor carpi radialis are the most commonly affected.
Golfer’s elbow is roughly 5 to 10 times less common than tennis elbow, accounting for about 10-20% of all epicondylar tendinopathies (Shiri et al., 2006, Am J Epidemiol). However, it can be more disabling because the medial elbow is intimately related to the ulnar nerve, which runs directly behind the medial epicondyle. Up to 50% of patients with golfer’s elbow have concurrent ulnar nerve irritation, producing tingling or numbness in the ring and little fingers.
What causes golfer’s elbow?
Repetitive wrist flexion, forearm pronation, and gripping are the mechanical drivers. Golf is an obvious culprit, particularly when grip pressure is excessive, technique is poor, or practice volume spikes suddenly. But plenty of other activities produce the same loading pattern.
Climbing, both rock climbing and indoor bouldering, is a common cause among younger patients. Weight training exercises like heavy barbell curls, deadlifts, and pull-ups load the medial elbow intensely. Trades that involve sustained gripping, hammering, or using vibrating tools are also high-risk. On the Costa del Sol, Costa Health frequently sees golfer’s elbow in padel players and golfers, particularly those who play multiple rounds per week without adequate conditioning.
The pathology mirrors tennis elbow. Histological examination shows degenerative tendon changes: disorganised collagen, neovascularisation, and increased ground substance rather than inflammatory cells. The term “epicondylitis” is therefore misleading. This is a degenerative overload problem, not an inflammatory one, and treating it as inflammation (with cortisone, rest alone, or ice) misses the mark.
What are the symptoms?
Pain and tenderness on the inner side of the elbow, directly over the medial epicondyle, is the primary complaint. Gripping forcefully, shaking hands, turning a screwdriver, or pouring from a kettle typically provokes it. The pain may radiate down the inner forearm toward the wrist.
Morning stiffness that loosens with gentle activity is characteristic. Grip strength is usually reduced, and patients often describe a “weakness” that makes them reluctant to grip firmly. In cases where the ulnar nerve is also involved, patients report tingling or numbness in the fourth and fifth fingers, particularly after sustained elbow flexion such as holding a phone to the ear or sleeping with the elbow bent.
One edge case worth noting: medial elbow pain in overhead throwing athletes (cricketers, javelin throwers) can indicate ulnar collateral ligament (UCL) stress rather than a pure tendinopathy. The treatment approach for UCL problems differs significantly, so accurate diagnosis is critical, especially in athletes planning to return to throwing sports.
How is golfer’s elbow treated?
Progressive tendon loading is the evidence-based first-line treatment. The principles are the same as for tennis elbow: the tendon needs gradually increasing mechanical load to stimulate collagen remodelling and restore capacity. Complete rest allows the tendon to decondition further, making symptoms worse when activity resumes.
Physiotherapy at Costa Health follows a structured progression. Daniele Delicati typically begins with isometric wrist flexion holds, which can provide immediate pain relief while initiating the loading process. Eccentric exercises, specifically slow, controlled wrist flexion lowering against resistance, form the next phase. Heavy slow resistance training, using higher loads at slower speeds, builds tendon resilience over 8 to 12 weeks.
Addressing the kinetic chain is essential. Poor thoracic rotation in golfers forces the wrists and forearms to compensate during the swing, overloading the medial elbow. Chiropractic and osteopathic assessment of the thoracic spine, shoulder, and wrist can identify stiffness and movement restrictions that contribute to excessive medial elbow loading. A golfer with a stiff thoracic spine and limited shoulder rotation will always overwork the forearms, regardless of how strong the flexor tendons become.
Sports massage for the forearm flexors, pronator teres, and the muscles of the hand helps manage tissue tightness and improve the mechanical environment around the medial epicondyle. Soft tissue work proximal to the elbow, addressing the biceps and anterior shoulder, is also relevant because tightness in these areas alters how force transmits through the arm.
Should you use a brace?
A medial counterforce strap worn just below the elbow can reduce the force transmitted to the tendon origin during gripping activities. It’s a useful symptom management tool during the rehabilitation period, particularly for people who can’t completely avoid provocative tasks at work. The strap doesn’t replace strengthening, but it can make activities more tolerable while the tendon rebuilds.
How long does recovery take?
Tendon remodelling is slow. Most patients see meaningful improvement within 6 to 12 weeks of consistent loading, but full resolution of a chronic golfer’s elbow can take 3 to 6 months. Compliance with the home exercise programme is the single most important factor influencing outcome. Patients who do the exercises consistently, even when symptoms start to improve, have significantly better long-term results than those who stop early.
When should someone seek help?
Inner elbow pain lasting beyond two weeks, pain that limits grip strength or daily activities, or any tingling or numbness in the ring and little fingers warrants professional assessment. Acute medial elbow pain after a specific throwing or lifting event, particularly in athletes, needs prompt evaluation to rule out UCL injury.
Costa Health’s clinics in Marbella and Riviera del Sol provide thorough assessment and evidence-based rehabilitation for golfer’s elbow. Book a consultation to start a structured recovery programme.