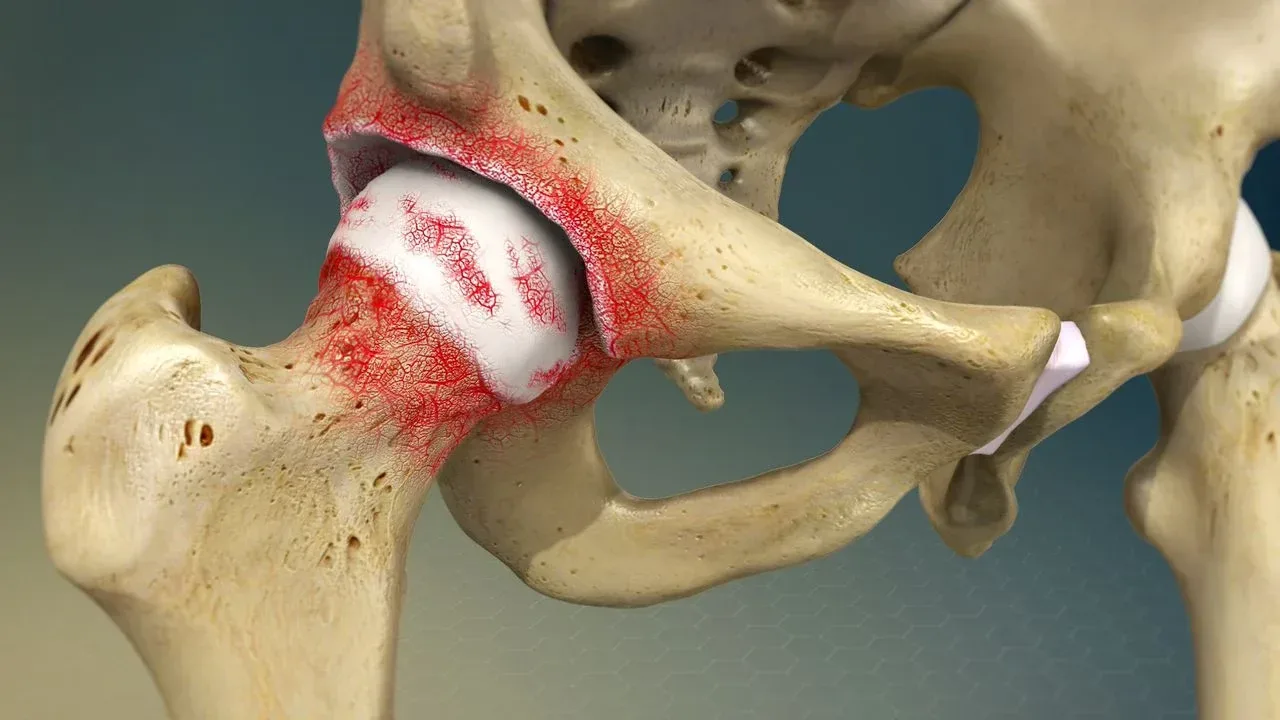

Degenerative joint disease of the hip, more commonly called hip osteoarthritis, is the gradual breakdown of the cartilage that lines the ball-and-socket joint between your femur and pelvis. It causes groin pain, morning stiffness, and a progressive loss of range that eventually makes everyday tasks like putting on shoes or getting out of a car genuinely difficult.
Who gets hip osteoarthritis, and how common is it?
Hip OA is one of the most prevalent musculoskeletal conditions worldwide. The Global Burden of Disease study (2019) estimated that over 300 million people live with osteoarthritis, with the hip being the second most affected joint after the knee. Age, genetics, previous hip injury, and excess body weight all increase the risk, but it isn’t exclusively a condition of older adults. Former athletes with femoroacetabular impingement (FAI) can develop significant cartilage loss in their 40s.
A clinical example illustrates the point. Paul Morrison, chiropractor at Costa Health, regularly treats expats on the Costa del Sol who assumed their “stiff hip” was just part of ageing. By the time they seek help the joint has often lost 30 or more degrees of internal rotation, the surrounding muscles have weakened, and compensatory back pain has developed. Earlier intervention wouldn’t have reversed the cartilage loss, but it would have slowed functional decline significantly.
Where exactly does hip OA hurt?
This is where many people get caught out. Hip osteoarthritis typically presents as groin pain, not lateral buttock pain. Patients often point to the front of their hip crease or the inner thigh. Pain at the side of the hip is more likely to be gluteal tendinopathy or trochanteric bursitis, two conditions that get misdiagnosed as hip OA surprisingly often.
Stiffness dominates in the early stages. Getting out of a chair after sitting for 30 minutes produces a few seconds of hobbling that eases once you get moving. As the disease progresses, that stiffness lingers longer and pain starts arriving during weight-bearing activities rather than just at the start of movement.
One misconception worth correcting: the severity of X-ray changes doesn’t reliably predict how much pain someone has. A study published in the Annals of the Rheumatic Diseases (2019) showed that roughly 40% of people with moderate-to-severe radiographic hip OA reported little or no pain. The clinical picture, not the image, should guide treatment decisions.
What can manual therapy do for a hip that’s wearing out?
Conservative management is the recommended first line of treatment for hip OA according to both NICE (2022) and EULAR guidelines, and that’s exactly where chiropractic, physiotherapy, osteopathy, and sports massage sit.
Joint mobilisation performed by a chiropractor or osteopath can temporarily restore accessory glide within the hip capsule, reduce pain, and improve functional range. It won’t regrow cartilage, but it can make a real difference to how the joint feels day to day.
Physiotherapy-led exercise is the single most evidence-backed intervention for hip OA outside of surgery. Strengthening the gluteal muscles, particularly gluteus medius, offloads the joint during walking and stair climbing. A 2014 Cochrane review confirmed that land-based therapeutic exercise reduces pain and improves physical function in hip OA, with benefits comparable to those of non-steroidal anti-inflammatory drugs but without the gastrointestinal side effects.
Sports massage and soft tissue work target the tight hip flexors, adductors, and piriformis that clamp down around an arthritic joint. Releasing these tissues reduces compressive load and often gives patients noticeably more freedom of movement within a single session.
When does hip OA need surgery?
Not every arthritic hip ends up in an operating theatre. Many patients manage well for years with structured exercise, weight management, and periodic manual therapy. The tipping point for joint replacement is pain that persists despite conservative care and significantly limits daily life.
If walking fewer than 500 metres is painful, if sleep is regularly disrupted by hip pain, or if you’ve stopped activities you value because the hip can’t cope, it’s worth discussing surgical referral with your clinician. Total hip replacement remains one of the most successful operations in medicine, with over 95% of patients reporting significant pain relief at 10 years post-op (National Joint Registry, 2023).
Is there anything you can do to slow the progression?
Three things make the biggest difference. Maintaining a healthy body weight reduces the mechanical load on the hip with every step. Staying active with low-impact exercise, swimming, cycling, and walking, preserves muscle strength and joint nutrition. And getting clinical guidance early means you can address biomechanical factors like pelvic asymmetry or gait compensation before they accelerate wear.
Costa Health’s team in Marbella works across disciplines to keep arthritic hips moving for as long as possible. If groin stiffness or hip pain is starting to limit your day, book an assessment and find out where you stand.