
De Quervain’s tenosynovitis is inflammation of the tendon sheath surrounding the abductor pollicis longus and extensor pollicis brevis tendons on the thumb side of the wrist. It causes pain when gripping, twisting, or moving the thumb, and it’s one of the most common causes of radial (thumb-side) wrist pain seen in clinical practice.
The condition is named after the Swiss surgeon Fritz de Quervain, who described it in 1895. More than a century later, it remains frequently misdiagnosed or dismissed as a minor strain. It isn’t minor for the person who can’t turn a door handle, pick up a kettle, or hold their baby without sharp, shooting pain at the wrist.
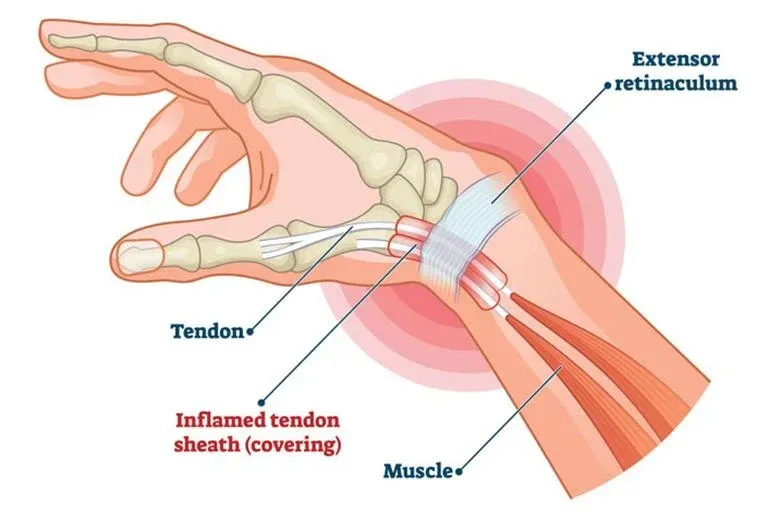
What’s happening inside the wrist?
Two tendons travel through a narrow tunnel, called the first dorsal compartment, on the thumb side of the wrist. This tunnel is lined with a synovial sheath that produces fluid to allow smooth gliding. When repetitive thumb and wrist movements irritate this sheath, it swells. The swollen sheath narrows the tunnel, and the tendons can no longer glide freely. Every thumb movement then creates friction, pain, and sometimes an audible or palpable catching sensation.
In some people, an anatomical variant creates a septum (dividing wall) within the first dorsal compartment, effectively splitting it into two sub-tunnels. Research published in the Journal of Hand Surgery European Volume found this variant present in approximately 28% of cadaveric specimens (Mirzanli et al., 2012). This anatomical quirk is clinically significant because it can make the condition more resistant to standard treatments, including corticosteroid injections that may only reach one of the two sub-compartments.
Who gets De Quervain’s?
New parents are the classic demographic. Repeatedly lifting an infant with thumbs extended and wrists deviated places enormous strain on the first dorsal compartment. The condition’s informal name, “mummy thumb” or “mother’s wrist,” reflects this, though fathers and grandparents develop it just as readily.
Hormonal changes during pregnancy and the postpartum period also play a role. Fluid retention during pregnancy increases soft tissue swelling, and the relaxin hormone that loosens ligaments for childbirth may affect tendon sheath integrity. A study by Avci et al. in the European Journal of Obstetrics & Gynecology (2002) found that De Quervain’s prevalence was significantly elevated in the third trimester and postpartum period.
Beyond new parents, the condition affects anyone performing repetitive thumb and wrist movements. Smartphone users (the term “texting thumb” has entered the clinical vocabulary), gamers, musicians, hairdressers, and craftspeople all present regularly. Sarah Monaghan, Costa Health’s principal chiropractor, notes that the Costa del Sol’s golf and padel communities are frequent sufferers, given the repetitive grip demands of both sports.
One firm clinical position worth stating: the condition won’t resolve if the aggravating activity continues unmodified. Rest from the specific provocative movement is non-negotiable in the early stages.
How is it diagnosed?
The Finkelstein test is the classic diagnostic manoeuvre. The patient makes a fist with the thumb tucked inside the fingers, then the examiner deviates the wrist towards the little finger side. Sharp pain over the radial styloid (the bony bump on the thumb side of the wrist) confirms the diagnosis. A modified Eichhoff test, where the patient performs the ulnar deviation actively, is now preferred by some clinicians as it’s slightly more specific.
Imaging is rarely needed. Ultrasound can show thickening of the tendon sheath and increased fluid within the first dorsal compartment if diagnostic confirmation is required or if the clinician suspects the septated anatomical variant.
An important differential to rule out: intersection syndrome, which produces pain slightly higher on the forearm (about four centimetres proximal to Lister’s tubercle) and involves a different set of tendons. The two conditions are sometimes confused, but their treatment approaches differ.
What does treatment involve?
De Quervain’s responds well to conservative management when caught early. Costa Health takes a multidisciplinary approach using chiropractic, physiotherapy, osteopathy, and sports massage because the wrist doesn’t function in isolation from the rest of the upper limb.
Splinting is often the first step. A thumb spica splint immobilises the thumb and wrist, removing the repetitive stress that drives the inflammation. Wearing it for two to four weeks, particularly during provocative activities, allows the tendon sheath to settle.
Physiotherapy introduces graded tendon-gliding exercises once acute pain subsides. Isometric thumb exercises, progressed to eccentric loading, help the tendons adapt to controlled stress. Wrist extensor and flexor stretching maintains range of motion while the area heals. Physiotherapists at Costa Health also address ergonomic factors: how the patient holds their phone, carries their child, or grips their padel racquet.
Chiropractic assessment looks beyond the wrist. Restrictions in the radiocarpal, midcarpal, and carpometacarpal joints alter movement mechanics and increase tendon strain. Mobilisation of these joints restores normal biomechanics. Assessment of the elbow, shoulder, and cervical spine identifies upstream contributors, a stiff thoracic spine or restricted shoulder can cause compensatory overuse patterns at the wrist.
Osteopathic treatment examines the fascial continuity from the cervical spine through the shoulder, elbow, and forearm to the wrist. Myofascial release of the forearm extensor compartment reduces the mechanical tension on the first dorsal compartment. Lymphatic drainage techniques can help reduce local swelling.
Sports massage targets the forearm extensors, thenar eminence, and intrinsic hand muscles. Soft tissue work through the extensor compartment relieves chronic tension that perpetuates the condition, while careful cross-fibre massage over the first dorsal compartment encourages tendon sheath healing.
When should you seek urgent care?
De Quervain’s itself isn’t dangerous, but wrist pain with additional features needs prompt investigation. Numbness or tingling in the thumb, index, or middle fingers suggests possible carpal tunnel syndrome, a different condition requiring different management. Sudden inability to extend the thumb after a fall may indicate a tendon rupture or scaphoid fracture. Redness, heat, and swelling with fever could indicate infection of the tendon sheath (septic tenosynovitis), which is a surgical emergency.
What’s the recovery outlook?
Most patients improve significantly within six to eight weeks of consistent conservative treatment. Around 80% of cases resolve without the need for corticosteroid injection. Cases that don’t respond to conservative care within three months are typically referred for injection or, rarely, surgical release of the first dorsal compartment.
Recurrence is common if the underlying cause isn’t addressed. That means ongoing attention to grip technique, workstation ergonomics, and gradual return to provocative activities. Costa Health’s team can build a recovery plan that addresses both the immediate pain and the long-term prevention strategy, drawing on chiropractic, physiotherapy, and sports massage as needed.