
Achilles tendonitis is inflammation or irritation of the Achilles tendon, the strongest tendon in the body, connecting the calf muscles to the heel bone. It produces pain at the back of the ankle or lower calf that worsens with activity, and it affects roughly 6% of the general population at some point in their lives.
The Achilles tendon handles forces of up to 12.5 times body weight during running, according to research published in the Journal of Biomechanics (Komi et al., 1992). That extraordinary load capacity is precisely what makes it vulnerable. When the tendon is asked to do more than it’s conditioned for, tissue damage outpaces repair, and pain follows.
What’s the difference between tendonitis and tendinopathy?
Terminology matters here. Acute Achilles tendonitis involves genuine inflammatory cells and usually responds to anti-inflammatory measures. Chronic Achilles tendinopathy, which is far more common in clinical practice, involves degenerative changes within the tendon’s collagen structure with minimal actual inflammation. A 2019 consensus statement in the British Journal of Sports Medicine recommended the umbrella term “Achilles tendinopathy” because most presentations are degenerative rather than inflammatory by the time a patient seeks treatment.
Sarah Monaghan, Costa Health’s principal chiropractor with over 20 years of clinical experience, sees this distinction play out weekly. Patients arrive having iced and rested for months, frustrated that the pain hasn’t budged. Ice reduces inflammation. But if inflammation isn’t the primary problem, ice alone won’t fix it.
Who develops Achilles tendonitis?
Runners account for the largest single group, but they’re far from the only ones affected. Weekend tennis players, padel enthusiasts (extremely common on the Costa del Sol), hikers, and dancers all present regularly. A sudden increase in training volume is the classic trigger. Going from sedentary to a holiday hiking programme, or jumping into a new sport without graduated loading, overwhelms the tendon’s adaptive capacity.
Age is a significant risk factor. Tendon vascularity decreases after 30, slowing repair. Tight calf muscles, flat feet, and excessive pronation all increase mechanical stress on the tendon. Certain medications, notably fluoroquinolone antibiotics, carry a well-documented risk of Achilles tendon damage and even rupture.
One clinical example Costa Health sees repeatedly: expats who move to southern Spain from cooler climates and switch from supportive winter boots to flat sandals while simultaneously increasing their walking on hilly terrain. That combination of reduced heel height, altered biomechanics, and increased activity is a reliable recipe for Achilles problems.
Where exactly does it hurt?
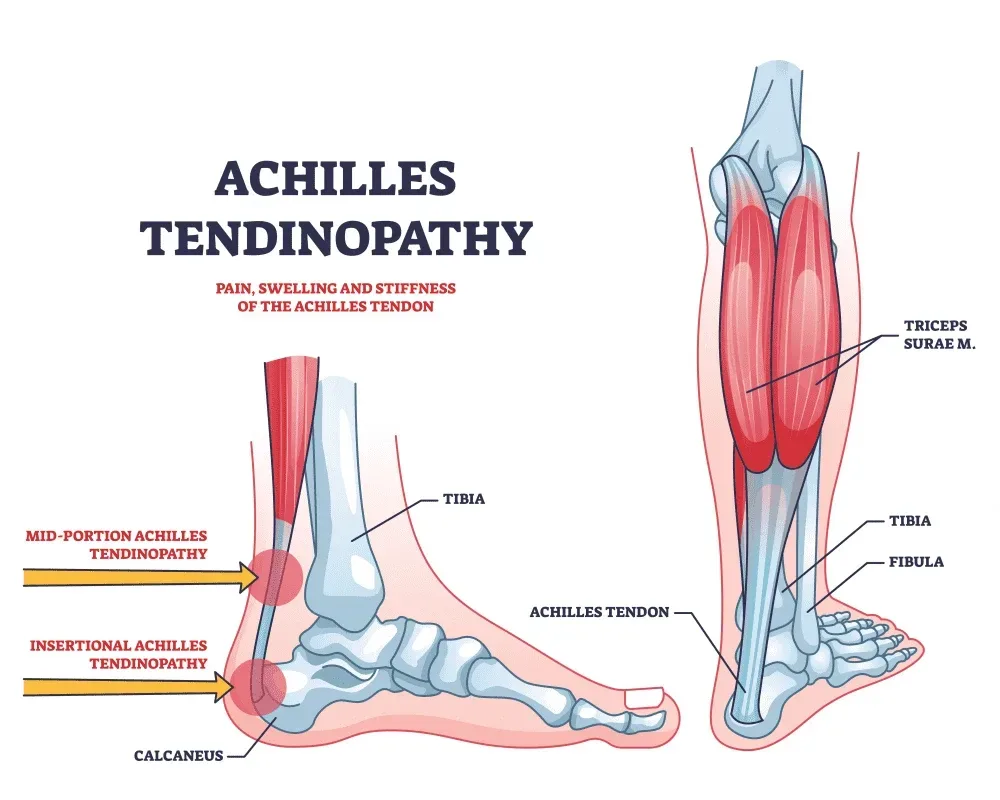
Achilles tendonitis presents in two distinct patterns. Midportion tendinopathy, the more common form, produces pain and thickening two to six centimetres above the heel bone insertion. Insertional tendinopathy causes pain exactly where the tendon attaches to the calcaneus and is often associated with a bony prominence called a Haglund’s deformity.
The distinction matters because treatment protocols differ. Midportion tendinopathy responds exceptionally well to eccentric loading exercises. Insertional tendinopathy often doesn’t tolerate those same exercises in their standard form and needs modified loading positions.
Morning stiffness is the hallmark of both types. The tendon stiffens overnight, and those first few steps out of bed produce a characteristic ache that eases within minutes of walking. Pain during or after activity, warmth over the tendon, and sometimes a palpable nodule within the tendon body complete the picture.
How does Costa Health treat Achilles tendonitis?
Effective treatment requires more than rest. The tendon needs progressive, controlled loading to stimulate collagen remodelling and restore tensile strength. Costa Health’s team draws on chiropractic, physiotherapy, osteopathy, and sports massage to build a treatment plan around each individual’s presentation.
Eccentric exercise programmes, originally described by Alfredson et al. (1998) and since validated by the 2024 clinical practice guidelines from the Academy of Orthopaedic Physical Therapy, remain a cornerstone of Achilles tendinopathy treatment. Current evidence supports progressive tendon loading, whether eccentric, concentric-eccentric, or heavy slow resistance, rather than a single protocol. Costa Health’s physiotherapists prescribe and progress these exercises based on individual tolerance and response.
Chiropractic assessment identifies joint restrictions in the ankle, subtalar joint, and foot that alter load distribution through the Achilles. Restoring normal dorsiflexion range at the talocrural joint reduces compensatory stress on the tendon. Biomechanical assessment of gait and footwear forms a core part of this approach.
Osteopathic treatment examines the kinetic chain from the lumbar spine through the pelvis, hip, knee, and ankle. Restrictions anywhere upstream can alter calf muscle mechanics and increase tendon loading. Fascial release through the posterior compartment of the lower leg often provides measurable improvements in range of motion within a single session.
Sports massage addresses chronic tension in the gastrocnemius and soleus muscles that maintains excessive resting tension on the tendon. Deep tissue work and instrument-assisted soft tissue mobilisation help break down adhesions and restore tissue pliability.
When is Achilles tendon pain something more serious?
Most Achilles tendon pain is a nuisance, not an emergency. But sudden, severe pain at the back of the ankle accompanied by a “pop” or the sensation of being kicked in the calf warrants immediate medical attention. This presentation suggests a partial or complete Achilles tendon rupture, which may require surgical repair. Thompson’s squeeze test (squeezing the calf while the patient lies prone) can quickly distinguish a rupture from tendinopathy, and it’s something any qualified practitioner should perform when the history raises suspicion.
Bilateral Achilles tendon pain in a patient taking fluoroquinolone antibiotics should also prompt immediate cessation of the medication and medical review. The FDA issued a boxed warning on this drug class specifically because of the tendon rupture risk.
How long until you’re back to full activity?
Mild cases caught within the first few weeks often improve within six to eight weeks of structured treatment. Chronic cases that have been present for months typically need three to six months of consistent rehabilitation. Returning to sport too quickly is the most common reason for relapse. Graduated return-to-activity protocols, where load is increased by no more than 10% per week, give the remodelling tendon the best chance of tolerating full activity without setback.
Costa Health’s multidisciplinary approach means treatment adapts as you progress. What you need in week one is different from what you need in week eight, and having chiropractic, physiotherapy, and sports massage available under one roof makes that transition straightforward for patients on the Costa del Sol.